Ebola resurfaces across central Africa
2026-05-16
Shock comes late. Confirmation of Ebola outbreaks in Congo and Uganda arrived only after suspected infections climbed to 246 and deaths reached 65, according to health officials. WHO first learned of potential cases on May 5, yet the US Centers for Disease Control and Prevention has said it was informed only yesterday, a delay that would unsettle any epidemic modeler.
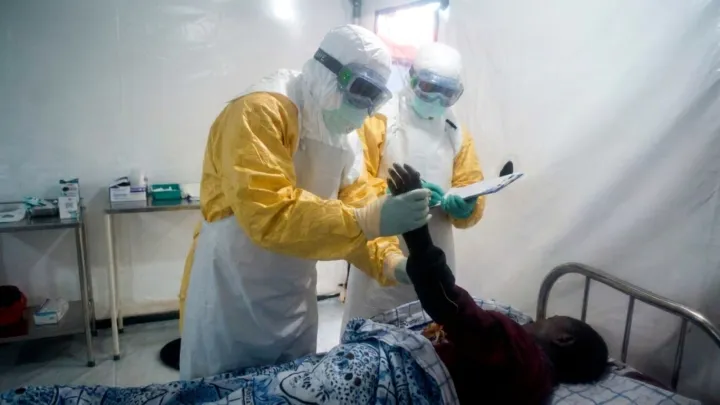
This reporting lag is not a minor bureaucratic glitch. In Ebola control, every unreported chain of transmission means more viral replication, more exposure, and more pressure on already thin infection‑prevention systems, from isolation wards to contact tracing teams. Hemorrhagic fever outbreaks turn on basic epidemiology: rapid case definition, strict barrier nursing, and aggressive surveillance of close contacts. When international agencies receive staggered alerts, coordination of laboratory confirmation, personal protective equipment stockpiles, and clinical protocols becomes fragmented.
The geography is no surprise, and that is the problem. Cross‑border movement between Congo and Uganda, dense informal trade routes, and limited intensive‑care capacity create ideal conditions for Ebola to spread before authorities can enforce quarantine or safe‑burial procedures. Viral load peaks early; so does risk to health workers without consistent access to negative‑pressure rooms or reliable diagnostics such as polymerase chain reaction assays. The numbers released so far may represent only the visible portion of a wider transmission network.
Loading...

